 Get Immediate Access To Your Special Report And Top Tips From Our PTs!
Get Immediate Access To Your Special Report And Top Tips From Our PTs!
Introduction
Physiotherapy in Redcliffe for Mid Back
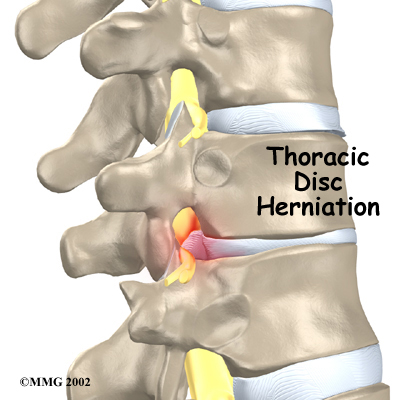
Few people with a thoracic disc herniation feel any symptoms or have any problems as a result of this condition. In rare cases when symptoms do arise, the main concern is whether the herniated disc is affecting the spinal cord.
Although people often refer to a thoracic disc herniation as a slipped disc, the disc doesn't actually slip out of place. Rather, the term herniation means that the material in the center of the disc has squeezed out of the normal space. In the thoracic spine, this condition mostly affects people between 40 and 60 years old.
This guide will help you understand:
- how the problem develops
- how doctors diagnose the condition
- what treatment options are available
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Back Pain|limit:15|heading:Hear from some of our patients who we treated for *Back Pain*#
Anatomy
What parts of the spine are involved?
The human spine is formed by 24 spinal bones, called vertebrae. Vertebrae are stacked on top of one another to create the spinal column. The main section of each vertebra is a round block of bone, called the vertebral body.
Spinal Column
 The thoracic spine is made up of the middle 12 vertebrae. Doctors often refer to these vertebrae as T1 to T12. The thoracic spine starts at the base of the neck. The lowest vertebra of the thoracic spine, T12, connects below the bottom of the rib cage to the first vertebra of the lumbar spine, called L1.
The thoracic spine is made up of the middle 12 vertebrae. Doctors often refer to these vertebrae as T1 to T12. The thoracic spine starts at the base of the neck. The lowest vertebra of the thoracic spine, T12, connects below the bottom of the rib cage to the first vertebra of the lumbar spine, called L1.
Thoracic Spine
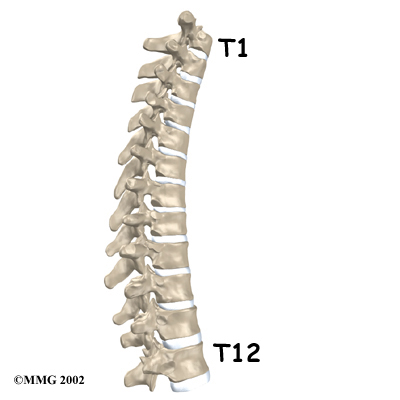
 The upper half of the thoracic spine is much less mobile than the lower section, making disc herniations in the upper thoracic spine rare. About 75 percent of thoracic disc herniations occur from T8 to T12, with the majority affecting T11 and T12.
The upper half of the thoracic spine is much less mobile than the lower section, making disc herniations in the upper thoracic spine rare. About 75 percent of thoracic disc herniations occur from T8 to T12, with the majority affecting T11 and T12.
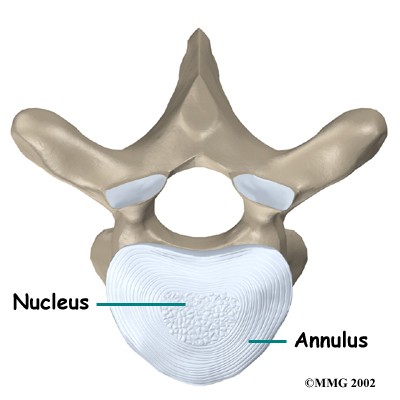
The intervertebral disc is a specialized connective tissue structure that separates the vertebral bodies. The disc is made of two parts. The center, called the nucleus, is spongy. It provides most of the disc's ability to absorb shock. The nucleus is held in place by the annulus, a series of ligament rings surrounding it. Ligaments are strong connective tissues that attach bones to other bones.
Healthy discs work like shock absorbers to cushion the spine. They protect the spine against the daily pull of gravity and during activities that put strong force on the spine, such as jumping, running, and lifting.
The spinal canal is a hollow tube inside the spinal column. It surrounds the spinal cord as it passes through the spine. The spinal cord is similar to a long wire made up of millions of nerve fibers. Just as the skull protects the brain, the bones of the spinal column protect the spinal cord. The spinal canal is narrow in the thoracic spine. Any condition that takes up extra space inside this canal can injure the spinal cord.
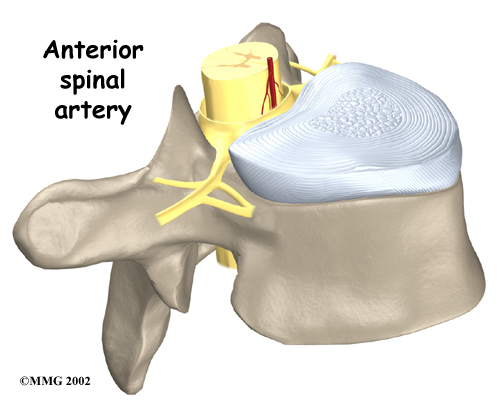
Blood vessels that run up and down the spine nourish the spinal cord. However, only one vessel, the anterior spinal artery, goes to the front of the spinal cord in the area between T4 and T9. Doctors call this section of the spine the critical zone. If this single vessel is damaged, as can happen with pressure from a herniated thoracic disc, the spinal cord has no other way to get blood. Left untreated, this section of the spinal cord dies, which can lead to severe problems of weakness or paralysis below the waist.
Anterior Spinal Artery
Related Document: My Health Team's Guide to Thoracic Spine Anatomy
Causes
Why do I have this problem?
Thoracic disc herniations are mainly caused by wear and tear in the disc. This wear and tear is known as degeneration. As a disc's annulus ages, it tends to crack and tear. These injuries are repaired with scar tissue. Over time the annulus weakens, and the nucleus may squeeze (herniate) through the damaged annulus. Spine degeneration is common in T11 and T12. T12 is where the thoracic and lumbar spine meet. This link is subject to forces from daily activity, such as bending and twisting, which lead to degeneration. Not surprisingly, most thoracic disc herniations occur in this area.
 Less commonly, a thoracic disc may herniate suddenly (an acute injury). A thoracic disc may herniate during a car accident or a fall. A thoracic disc may also herniate as a result of a sudden and forceful twist of the mid-back.
Less commonly, a thoracic disc may herniate suddenly (an acute injury). A thoracic disc may herniate during a car accident or a fall. A thoracic disc may also herniate as a result of a sudden and forceful twist of the mid-back.
Diseases of the thoracic spine may lead to thoracic disc herniation. Patients with Scheuermann's disease, for example, are more likely to suffer thoracic disc herniations. It appears these patients often have more than one herniated disc, though the evidence is not conclusive.
Related Document: My Health Teams Guide to Scheuermann's Disease (also known as Kyphosis)
The spinal cord may be injured when a thoracic disc herniates. The spinal canal of the thoracic spine is narrow, so the spinal cord is immediately in danger from anything that takes up space inside the canal. Most disc herniations in the thoracic spine squeeze straight back, rather than deflecting off to either side. As a result, the disc material is often pushed directly toward the spinal cord. A herniated disc can cut off the blood supply to the spinal cord. Discs that herniate into the critical zone of the thoracic spine (T4 to T9) can shut off blood from the one and only blood vessel going to the front of the spinal cord in this section of the spine. This can cause the nerve tissues in the spinal cord to die, leading to severe problems of weakness or paralysis in the legs.
Symptoms
What does the condition feel like?
Symptoms of thoracic disc herniation vary widely. Symptoms depend on where and how big the disc herniation is, where it is pressing, and whether the spinal cord has been damaged.
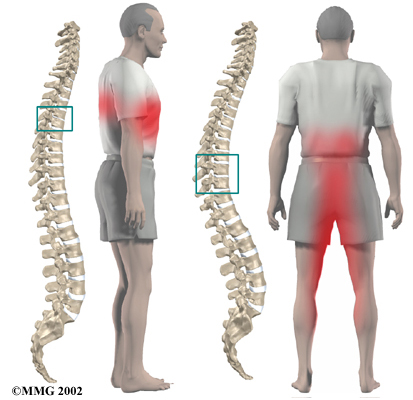
Pain is usually the first symptom. The pain may be centered over the injured disc but may spread to one or both sides of the mid-back. Also, patients commonly feel a band of pain that goes around the front of the chest. Patients may eventually report sensations of pins, needles, and numbness. Others say their leg or arm muscles feel weak. Disc material that presses against the spinal cord can also cause changes in bowel and bladder function.
Disc herniations can affect areas away from the spine. Herniations in the upper part of the thoracic spine can radiate pain and other sensations into one or both arms. If the herniation occurs in the middle of the thoracic spine, pain can radiate to the abdominal or chest area, mimicking heart problems. A lower thoracic disc herniation can cause pain in the groin or lower limbs and can mimic kidney pain.
Diagnosis
How do doctors diagnose the problem?
Diagnosis begins with a complete history and physical examination. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. These include questions about where you feel pain, if you have numbness or weakness in your arms or legs, and if you are having any problems with bowel or bladder function. Your doctor will also want to know what positions or activities make your symptoms worse or better.
Then the doctor examines you to see which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested.
X-rays show the bones. They normally don't show the discs, unless one or more of the discs have calcified. This is significant in the diagnosis of thoracic disc herniation. A calcified disc that appears on X-ray to poke into the spinal canal is a fairlyreliable sign that the disc has herniated. It isn't clear why a problem thoracic disc sometimes hardens from calcification, though past injury of the disc is one possibility.
The best way to diagnose a herniated thoracic disc is with magnetic resonance imaging (MRI). The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. It gives a clear picture of the discs and whether one has herniated. This machine creates pictures that look like slices of the area your doctor is interested in. The test does not require dye or a needle. This test has shown doctors that many people without symptoms have thoracic disc herniations. This has led some doctors to suggest that thoracic disc herniations not causing symptoms are normal.
Before MRI, doctors relied mainly on myelography to diagnose thoracic disc herniations. By itself, myelography only helps diagnose this condition in about half the cases. Myelography is a kind of X-ray test. A special dye is injected into the space around the spinal canal. The dye shows up on an X-ray. It helps a doctor see if the disc is pushing into the spinal canal.
Computed tomography (CT scan) may be ordered. This is a detailed X-ray that lets doctors see the body's tissue in images that also look like slices. The images provide more information about calcified discs. Doctors may combine the CT scan with myelography. When the CT scan is performed, the myelography dye highlights the spinal cord and nerves. The dye can improve the accuracy of a standard CT scan for diagnosing a herniated thoracic disc.
Doctors rely mostly on MRI for diagnosing thoracic disc herniations. However, they may use myelography and CT scans when preparing to do surgery to fix a herniated thoracic disc.
Treatment
What treatment options are available?
Nonsurgical Treatment
Doctors closely monitor patients with symptoms from a thoracic disc herniation, even when the size of the herniation is small. If the disc starts to put pressure on the spinal cord or on the blood vessels going to the spinal cord, severe neurological symptoms can develop rapidly. In these cases, surgery is needed right away. However, unless your condition is affecting the spinal cord or is rapidly getting worse, most doctors will begin with nonsurgical treatment.
At first, your doctor may recommend immobilizing your back. Keeping the back still for a short time can calm inflammation and pain. This might include one to two days of bed rest, since lying on your back can take pressure off sore discs and nerves. However, most doctors advise against strict bed rest and prefer their patients do ordinary activities, using pain to gauge how much activity is too much. Another option for immobilizing the back is a back support brace worn for up to one week.
Doctors prescribe certain types of medication for patients with thoracic disc herniation. Patients may be prescribed anti-inflammatory medications such as aspirin or ibuprofen. Muscle relaxants may be prescribed if the back muscles are in spasm. Pain that spreads into the arms or legs is sometimes relieved with oral steroids taken in tapering dosages.
Your doctor will probably have a physiotherapist direct your rehabilitation program. Physiotherapy treatments focus on relieving pain, improving back movement, and fostering healthy posture. A physiotherapist can design a rehabilitation program for your condition that helps you prevent future problems.
Most people with a herniated thoracic disc get better without surgery. Doctors usually have their patients try nonoperative treatment for at least six weeks before considering surgery.
My Health Team provides services for physiotherapy in Redcliffe.
Surgery
Surgeons may recommend surgery if patients aren't getting better with nonsurgical treatment, or if the problem is becoming more severe.
When there are signs that the herniated disc is affecting the spinal cord, surgery may be required, sometimes right away. The signs surgeons watch for when reaching this decision include weakening in the arm or leg muscles, pain that won't ease up, and problems with the bowels or bladder.
Surgical treatment for this condition includes
- costotransversectomy and discectomy
- transthoracic decompression
- video assisted thoracoscopy surgery (VATS)
- fusion
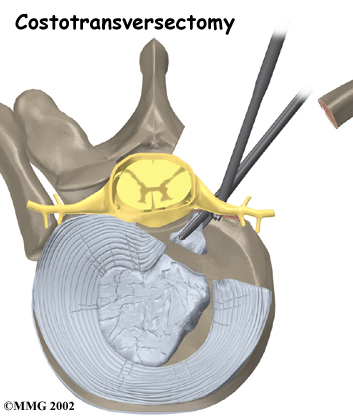
Costotransversectomy
Surgeons use costotransversectomy to open a window through the bones that cover the injured disc. Operating from the back of the spine, the surgeon takes out a small section on the end of two or more ribs where they connect to the spine. (Costo means rib.) Then the bony knob on the side of the vertebra (the transverse process) is removed. (Ectomy means to remove.) This opens a space for the surgeon to work. The injured portion of the disc that is pressing against the spinal cord is removed (discectomy) with small instruments. Surgeons take extreme care not to harm the spinal cord.
Transthoracic Decompression
Transthoracic describes the approach used by the surgeon. Trans means across or through. The thoracic region is the chest. So in transthoracic decompression, the surgeon operates through the chest cavity to reach the injured disc. This approach gives the surgeon a clear view of the disc.
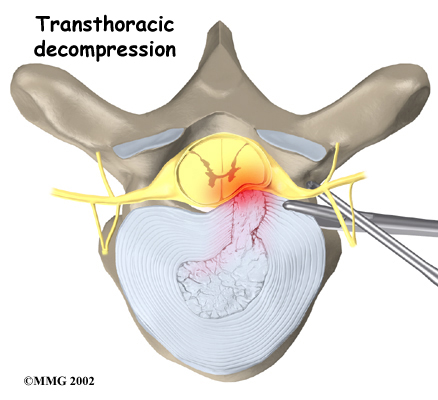
With the patient on his or her side, the surgeon cuts a small opening through the ribs on the side of the thorax (the chest). Instruments are placed through the opening, and the herniated part of the disc is taken out. This takes pressure off the spinal cord (decompression).
Video Assisted Thoracoscopy Surgery (VATS)
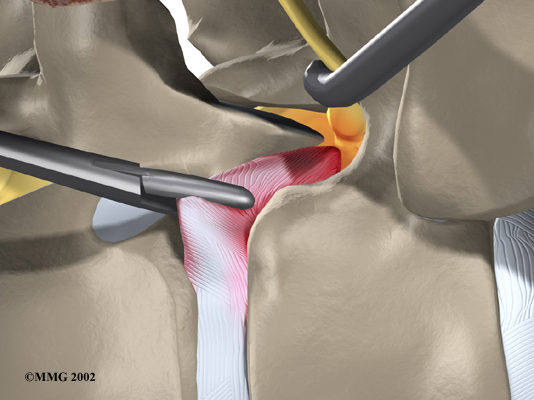
Recent developments in thoracic surgery include video assisted thoracoscopy surgery (VATS). This procedure is done with a thoracoscope, a tiny television camera that can be inserted into the side of the thorax through a small incision. The camera allows the surgeon to see the area where he or she is working on a TV screen. Small incisions give passage for other instruments used during the surgery. The surgeon watches the TV screen while cutting and removing damaged portions of the disc.
TV Screen
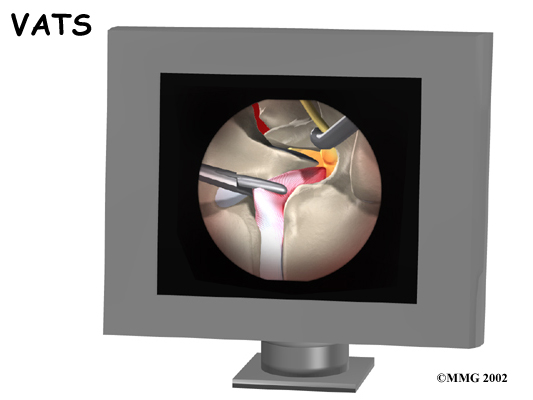
Cutting and Removing Damaged Portions
Categorized as minimally invasive surgery, VATS is thought to be less taxing on patients. Advocates also believe that this type of surgery is easier to perform, prevents scarring around the nerves and joints, and helps patients recover more quickly.
Fusion
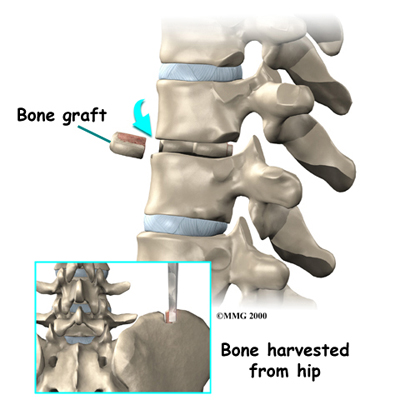
After removing part or all of the disc, the spine may be loose and unstable. Fusion surgery may be needed immediately afterward. The medical term for fusion is arthrodesis. This procedure locks the vertebrae in place and stops movement between the vertebrae. This steadies the bones and can ease pain. Fusion surgery is not usually needed if only a small amount of bone and disc material was removed during surgery to fix a herniated thoracic disc.
In this procedure, the surgeon lays small grafts of bone over or between the loose spinal bones. Surgeons may use a combination of screws, cables, and rods to prevent the vertebrae from moving and allow the graft to heal.
Rehabilitation
What should I expect as I recover?
Nonsurgical Rehabilitation
Even if you don't need surgery, your doctor may recommend that you work with a physiotherapist. Patients are normally seen a few times each week for four to six weeks.
The first goals of treatment are to control symptoms, find positions that ease pain, and teach you how to keep your spine safe during routine activities.
As patients recover, they gradually advance in a series of strengthening exercises. Aerobic exercises, such as walking or swimming, can ease pain and improve endurance.
After Surgery
Rehabilitation after surgery is more complex. Some patients leave the hospital shortly after surgery. However, some surgeries require patients to stay in the hospital for a few days. Patients who stay in the hospital may be visited by a physiotherapist soon after surgery. The treatment sessions help patients learn to move and do routine activities without putting extra strain on the back.
During recovery from surgery, patients should follow their surgeon's instructions about wearing a back brace or support belt. They should be cautious about overdoing activities in the first few weeks after surgery.
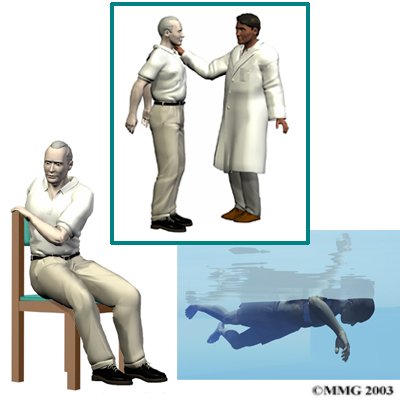
Many surgical patients need physiotherapy outside of the hospital. They see a physiotherapist for one to three months, depending on the type of surgery. At first, physiotherapists may use treatments such as heat or ice, electrical stimulation, massage, and ultrasound to calm pain and muscle spasm. Then they teach patients how to move safely with the least strain on the healing back.
As patients recover, they gradually begin doing flexibility exercises for the hips and shoulders, and mobility and strengthening exercises to address the back muscles. Patients may also work with the physiotherapist in a pool. Patients progress with exercises to improve endurance, muscle strength, and body alignment.
As the rehabilitation program evolves, patients do more challenging exercises. The goal is to safely advance strength and function.
Ideally, patients are able to go back to their previous activities. However, some patients may need to modify their activities to avoid future problems.
When treatment is well under way, regular visits to the physiotherapist's office will end. The physiotherapist will continue to be a resource, but patients will be in charge of doing their exercises as part of an ongoing home program.
My Health Team provides services for physiotherapy in Redcliffe.
Portions of this document copyright MMG, LLC.
